Author(s)
Frank A Fanizza, PharmD, BCACP
Emily S Prohaska, PharmD, BCACP, BCGCP
Reviewed By
Emily Heil, PharmD, BCPS, BCIDP
Jamie Wagner, PharmD, BCPS
Stevenson B, Trevenen M, Klinken E, et al. Multicenter Australian Study to Determine Criteria for Low- and High-Risk Penicillin Testing in Outpatients. J Allergy Clin Immunol Pract. 2020;8(2):681-689.e3.
The Problem
Many, many, many patients report they have penicillin (PCN) allergy. But while nearly 10% report being allergic to PCN, fewer than 1% have a true allergy.1 And this hampers antimicrobial stewardship efforts because clinicians are often forced to turn to agents with a broader spectrum, that are more expensive, and more likely to cause adverse effects including the development of resistance. However, determining whether a patient has a true PCN allergy is time-consuming and expensive. Historically, patients were sent to an allergist for PCN allergy skin testing (PAST) followed by oral provocation challenge (OPC). Formal PCN allergy skin tests can be uncomfortable for patients. What if patients could skip past the skin test and receive a direct OPC instead? Direct OPC may not only increase patient willingness to be tested but also the feasibility of offering testing in primary care (and perhaps community pharmacy) settings.
What’s Known
Traditionally, PAST is a stepwise process of a skin scratch test followed by an intradermal test using normal saline (negative control), histamine (positive control), and prepared penicillin solution(s). A negative PAST result has a negative predictive value (NPV) greater than 95%. However, when combined with an oral challenge, the NPV is nearly 100%.2
Unfortunately, PAST has several limitations. The results can be difficult to interpret, the test is costly, most clinics don’t have the expertise to perform the test, and the test is very time consuming.3-5 Thus, researchers have recently begun to investigate whether the direct OPC can be used as an alternative method to safely and effectively rule out PCN allergy. In a study of 818 children with suspected amoxicillin allergy, 94.1% tolerated direct OPC, resulting in an NPV of 89.1%.6 In a retrospective observational study of Marine recruits with self-reported PCN allergy, 98.5% tolerated direct OPC.7 In both studies, reactions to OPC were mild in nature and primarily consisted of cutaneous reactions. There were no documented cases of anaphylaxis or other life-threatening reactions.
Criteria for determining who is at low risk and can safely undergo direct OPC are available.3 Low risk has been defined as a history of benign rash, benign somatic symptoms, or unknown reaction history to PCN occurring at least one year ago. Among 806 patients who met inclusion criteria and underwent direct OPC, 95.7% tolerated the test.3 Additionally, the American Academy of Allergy, Asthma, and Immunology (AAAAI), the Infectious Diseases Society of America (IDSA), and the Society for Healthcare Epidemiology of America (SHEA) acknowledge that direct OPC can be safely used in select patients.2 Although there is apparent consensus that OPC is safe in select patients, there is not a universal definition of “low risk.”
What’s New
A recent study sought to determine whether PCN allergies can be safely de-labeled using OPC alone and, if so, which patients would be good candidates for direct OPC testing.8 This multicenter (n=7) Australian study was conducted between February 2016 and May 2018. Eligible subjects were at least 16 years old and referred for PCN allergy assessment. Exclusion criteria were: history of severe non-IgE-mediated PCN allergy; incomplete previous PAST testing; no previous PCN exposure; met de-labeling criteria based on history alone (eg, vomiting after PCN ingestion); diagnosis of significant medical comorbidity including severe asthma, structural lung disease, or ischemic heart disease; or current pregnancy. Reaction severity was defined using the World Allergy Organization Systemic Allergic Reaction Grading System (grade 1 through 4, with 4 being the most severe).
Site-specific testing protocols were allowed. Reagents used to perform PAST included benzylpenicillin (6 mg/mL), amoxicillin (20 mg/mL), and the “culprit” PCN specific to the patient’s allergy. Five sites performed PAST with penicilloyl polylsysine and minor determinant mixture. Four sites used ampicillin (20 mg/mL). Patients who reacted to PAST did not proceed to OPC. The “culprit” PCN if known or amoxicillin was used for OPC. One or two step OPCs were allowed with a minimum of 30 minute observation between doses and a minimum of 60 minute observation after the final dose. All sites had emergency equipment and staff trained to manage anaphylaxis. Four sites discharged patients on an extended course of oral PCN to monitor for delayed reactions. All patients received telephone follow-up 3 to 7 days after PAST/OPC to monitor for delayed reactions.
Of 476 patient records reviewed, 447 met inclusion criteria. Mean subject age was 43 years (range 16 to 91 years); 63.8% were female. The “culprit” PCN was unknown in most cases (68.9%), followed by amoxicillin (21.9%), amoxicillin/clavulanate (7.4%), or other (1.8%). The most common allergic reaction was grade 1 rash only (58.6%). A majority of patients (76.5%) experienced the allergic reaction to PCN more than 5 years prior to testing.
Figure 1 displays results from subjects who underwent PAST and/or OPC; a total of 67 (15%) subjects had a positive result. In total, 161 (96.4%) subjects who underwent direct OPC and 219 (78.2%) who underwent PAST and OPC had their PCN allergy successfully de-labeled.
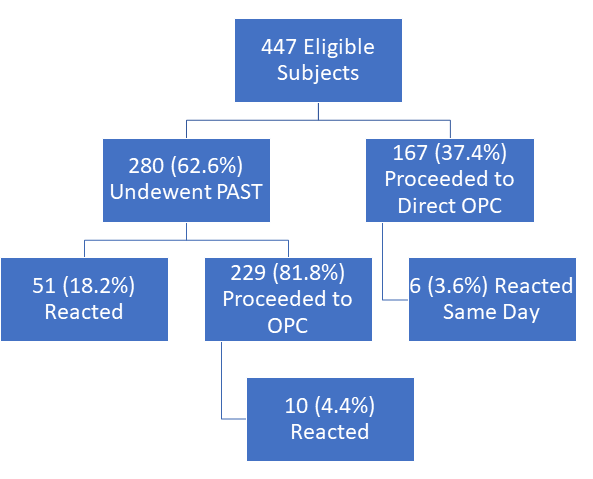
Figure 1: Test Results and Reactions. PAST: Penicillin Allergy Skin Testing. OPC: Oral Penicillin Challenge.
Eight low risk definitions were statistically modeled for optimal patient selection for direct OPC. Factors associated with a higher likelihood of positive reaction based on logistic regression included time since reaction (<1 year more likely) and grade of reaction (grade 4 more likely than grade 1 rash-only); no statistically significant differences were observed based on sex or age. The optimal statistically and clinically predictive low-risk definition tested was a history of grade 1 rash-only reaction to PCN that occurred more than one year prior to PAST/OPC; 244 (54.6%) subjects met this definition (sensitivity 80.6%, specificity 60.8%, NPV = 94.7%, C statistic 0.715).
Our Critical Appraisal
This trial is the first to publish an evidence-based definition for low-risk patients eligible for direct OPC using universally accepted definitions for classifying allergic reactions.9 While the study was multicenter (improving its generalizability), the study was limited to sites in Australia and testing protocols were not consistent between centers. Compared to other studies evaluating PCN allergy testing, the sample size was smaller.6,7
Joint guidelines published by AAAAI, IDSA, and SHEA define low-risk as a history of isolated reaction that was unlikely allergic, pruritus without rash, remote (>10 years ago) unknown reaction without features of IgE, and family history of PCN allergy.2 Kaiser Permanente in San Diego expanded “low-risk” criteria to include patients with benign somatic symptoms and unknown reaction to last PCN exposure.10 Among 806 patients who underwent direct OPC using this criteria, 4.2% developed a non-severe reaction to amoxicillin, which is slightly higher than the percentage of positive reactions to direct OPC found in the current study.2,10 However, results of this study should help to reassure clinicians, particularly non-allergists, that applying simple screening criteria is a safe and effective way to identify appropriate patients for direct oral PCN challenge.
The Bottom Line
Having a straightforward and evidence-based definition for low-risk patients eligible for direct OPC could increase the use of OPC and enhance our efforts to de-label patients who report a PCN allergy. While the current study’s criteria for “optimal low-risk” may under-represent patients who can safely proceed to direct OPC without PAST, this definition may provide comfort to non-allergist practices. Performing OPC and PCN allergy de-labeling activities in primary care settings is a valuable service that pharmacists, who are trained to skillfully collect medication histories, are perhaps uniquely qualified to provide.
The Key Points
- PCN allergy is frequently report but less than 1% have a true allergy; determining who can safely take PCN improves antimicrobial stewardship efforts
- Oral provocation challenge (OPC) testing can be safely conducted in primary care practices after appropriate patient screening
- Patients with a history of grade 1 rash-only reaction to PCN that occurred more than one year ago can proceed to direct OPC
FINAL NOTE: This program will be available for recertification credit through the American Pharmacists Association (APhA) Ambulatory Care Review and Recertification Program. To learn more, visit https://www.pharmacist.com/ambulatory-care-review-and-recertification-activities.
- Centers for Disease Control and Prevention. Evaluation and Diagnosis of Penicillin Allergy for Healthcare Professionals – Is it Really a Penicillin Allergy? https://www.cdc.gov/antibiotic-use/community/for-hcp/Penicillin-Allergy.html. Page last reviewed October 31, 2017. Accessed May 1, 2020.
- Joint Task Force on Practice Parameters representing the American Academy of Allergy, Asthma and Immunology; American College of Allergy, Asthma and Immunology; Joint Council of Allergy, Asthma and Immunology. Drug allergy: an updated practice parameter. Ann Allergy Asthma Immunol. 2010 Oct;105(4):259-273.
- Banks TA, Tucker M, Macy E. Evaluating Penicillin Allergies Without Skin Testing. Curr Allergy Asthma Rep. 2019;19(5):27.
- Shenoy ES, Macy E, Rowe T, Blumenthal KG. Evaluation and Management of Penicillin Allergy: A Review. JAMA. 2019;321(2):188-199.
- Blumenthal KG, Li Y, Banerji A, Yun BJ, Long AA, Walensky RP. The Cost of Penicillin Allergy Evaluation. J Allergy Clin Immunol Pract. 2018;6(3):1019-1027.e2.
- Mill C, Primeau MN, Medoff E, et al. Assessing the Diagnostic Properties of a Graded Oral Provocation Challenge for the Diagnosis of Immediate and Nonimmediate Reactions to Amoxicillin in Children. JAMA Pediatr. 2016;170(6):e160033.
- Tucker MH, Lomas CM, Ramchandar N, Waldram JD. Amoxicillin challenge without penicillin skin testing in evaluation of penicillin allergy in a cohort of Marine recruits. J Allergy Clin Immunol Pract. 2017;5(3):813-815.
- Stevenson B, Trevenen M, Klinken E, et al. Multicenter Australian Study to Determine Criteria for Low- and High-Risk Penicillin Testing in Outpatients. J Allergy Clin Immunol Pract. 2020;8(2):681-689.e3.
- Cox L, Larenas-linnemann D, Lockey RF, Passalacqua G. Speaking the same language: The World Allergy Organization Subcutaneous Immunotherapy Systemic Reaction Grading System. J Allergy Clin Immunol. 2010;125(3):569-74, 574.e1-574.e7.
- Aberer W, Macy E. Moving Toward Optimizing Testing for Penicillin Allergy. J Allergy Clin Immunol Pract. 2017;5(3):684-685.

 iForumRx.org is a web-based community of practice designed to inform ambulatory care pharmacy specialists, pharmacy residents, and student pharmacists about high-quality, practice-changing evidence.
iForumRx.org is a web-based community of practice designed to inform ambulatory care pharmacy specialists, pharmacy residents, and student pharmacists about high-quality, practice-changing evidence.